InVivoMAb anti-mouse CTLA-4 (CD152)
Product Description
Specifications
| Isotype | Syrian hamster IgG |
|---|---|
| Recommended Isotype Control(s) | InVivoMAb polyclonal Syrian hamster IgG |
| Recommended Dilution Buffer | InVivoPure pH 7.0 Dilution Buffer |
| Conjugation | This product is unconjugated. Conjugation is available via our Antibody Conjugation Services. |
| Immunogen | Mouse CTLA-4-human IgG1 fusion protein |
| Reported Applications |
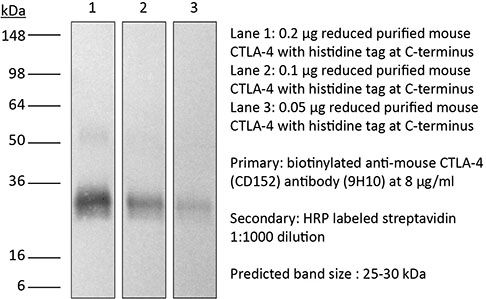
in vivo CTLA-4 neutralization in vitro CTLA-4 neutralization Western blot |
| Formulation |
PBS, pH 7.0 Contains no stabilizers or preservatives |
| Endotoxin |
≤1EU/mg (≤0.001EU/μg) Determined by LAL assay |
| Purity |
≥95% Determined by SDS-PAGE |
| Sterility | 0.2 µm filtration |
| Production | Purified from cell culture supernatant in an animal-free facility |
| Purification | Protein G |
| RRID | AB_10950184 |
| Molecular Weight | 150 kDa |
| Storage | The antibody solution should be stored at the stock concentration at 4°C. Do not freeze. |
| Need a Custom Formulation? | See All Antibody Customization Options |
Application References
-
Bartkowiak, T., et al (2015). "Unique potential of 4-1BB agonist antibody to promote durable regression of HPV+ tumors when combined with an E6/E7 peptide vaccine" Proc Natl Acad Sci U S A 112(38): E5290-5299.
PubMed
Antibody modulation of T-cell coinhibitory (e.g., CTLA-4) or costimulatory (e.g., 4-1BB) receptors promotes clinical responses to a variety of cancers. Therapeutic cancer vaccination, in contrast, has produced limited clinical benefit and no curative therapies. The E6 and E7 oncoproteins of human papilloma virus (HPV) drive the majority of genital cancers, and many oropharyngeal tumors. We discovered 15-19 amino acid peptides from HPV-16 E6/E7 for which induction of T-cell immunity correlates with disease-free survival in patients treated for high-grade cervical neoplasia. We report here that intranasal vaccination with these peptides and the adjuvant alpha-galactosylceramide elicits systemic and mucosal T-cell responses leading to reduced HPV(+) TC-1 tumor growth and prolonged survival in mice. We hypothesized that the inability of these T cells to fully reject established tumors resulted from suppression in the tumor microenvironment which could be ameliorated through checkpoint modulation. Combining this E6/E7 peptide vaccine with checkpoint blockade produced only modest benefit; however, coadministration with a 4-1BB agonist antibody promoted durable regression of established genital TC-1 tumors. Relative to other therapies tested, this combination of vaccine and alpha4-1BB promoted the highest CD8(+) versus regulatory FoxP3(+) T-cell ratios, elicited 2- to 5-fold higher infiltration by E7-specific CTL, and evoked higher densities of highly cytotoxic TcEO (T cytotoxic Eomesodermin) CD8 (>70-fold) and ThEO (T helper Eomesodermin) CD4 (>17-fold) T cells. These findings have immediate clinical relevance both in terms of the direct clinical utility of the vaccine studied and in illustrating the potential of 4-1BB antibody to convert therapeutic E6/E7 vaccines already in clinical trials into curative therapies.
-
Krummey, S. M., et al (2014). "Candida-elicited murine Th17 cells express high Ctla-4 compared with Th1 cells and are resistant to costimulation blockade" J Immunol 192(5): 2495-2504.
PubMed
Effector and memory T cells may cross-react with allogeneic Ags to mediate graft rejection. Whereas the costimulation properties of Th1 cells are well studied, relatively little is known about the costimulation requirements of microbe-elicited Th17 cells. The costimulation blocker CTLA-4 Ig has been ineffective in the treatment of several Th17-driven autoimmune diseases and is associated with severe acute rejection following renal transplantation, leading us to investigate whether Th17 cells play a role in CD28/CTLA-4 blockade-resistant alloreactivity. We established an Ag-specific model in which Th1 and Th17 cells were elicited via Mycobacterium tuberculosis and Candida albicans immunization, respectively. C. albicans immunization elicited a higher frequency of Th17 cells and conferred resistance to costimulation blockade following transplantation. Compared with the M. tuberculosis group, C. albicans-elicited Th17 cells contained a higher frequency of IL-17(+)IFN-gamma(+) producers and a lower frequency of IL-10(+) and IL-10(+)IL-17(+) cells. Importantly, Th17 cells differentially regulated the CD28/CTLA-4 pathway, expressing similarly high CD28 but significantly greater amounts of CTLA-4 compared with Th1 cells. Ex vivo blockade experiments demonstrated that Th17 cells are more sensitive to CTLA-4 coinhibition and therefore less susceptible to CTLA-4 Ig. These novel insights into the differential regulation of CTLA-4 coinhibition on CD4(+) T cells have implications for the immunomodulation of pathologic T cell responses during transplantation and autoimmunity.
-
Quezada, S. A., et al (2010). "Tumor-reactive CD4(+) T cells develop cytotoxic activity and eradicate large established melanoma after transfer into lymphopenic hosts" J Exp Med 207(3): 637-650.
PubMed
Adoptive transfer of large numbers of tumor-reactive CD8(+) cytotoxic T lymphocytes (CTLs) expanded and differentiated in vitro has shown promising clinical activity against cancer. However, such protocols are complicated by extensive ex vivo manipulations of tumor-reactive cells and have largely focused on CD8(+) CTLs, with much less emphasis on the role and contribution of CD4(+) T cells. Using a mouse model of advanced melanoma, we found that transfer of small numbers of naive tumor-reactive CD4(+) T cells into lymphopenic recipients induces substantial T cell expansion, differentiation, and regression of large established tumors without the need for in vitro manipulation. Surprisingly, CD4(+) T cells developed cytotoxic activity, and tumor rejection was dependent on class II-restricted recognition of tumors by tumor-reactive CD4(+) T cells. Furthermore, blockade of the coinhibitory receptor CTL-associated antigen 4 (CTLA-4) on the transferred CD4(+) T cells resulted in greater expansion of effector T cells, diminished accumulation of tumor-reactive regulatory T cells, and superior antitumor activity capable of inducing regression of spontaneous mouse melanoma. These findings suggest a novel potential therapeutic role for cytotoxic CD4(+) T cells and CTLA-4 blockade in cancer immunotherapy, and demonstrate the potential advantages of differentiating tumor-reactive CD4(+) cells in vivo over current protocols favoring in vitro expansion and differentiation.
-
Twyman-Saint Victor, C., et al (2015). "Radiation and dual checkpoint blockade activate non-redundant immune mechanisms in cancer" Nature 520(7547): 373-377.
PubMed
Immune checkpoint inhibitors result in impressive clinical responses, but optimal results will require combination with each other and other therapies. This raises fundamental questions about mechanisms of non-redundancy and resistance. Here we report major tumour regressions in a subset of patients with metastatic melanoma treated with an anti-CTLA4 antibody (anti-CTLA4) and radiation, and reproduced this effect in mouse models. Although combined treatment improved responses in irradiated and unirradiated tumours, resistance was common. Unbiased analyses of mice revealed that resistance was due to upregulation of PD-L1 on melanoma cells and associated with T-cell exhaustion. Accordingly, optimal response in melanoma and other cancer types requires radiation, anti-CTLA4 and anti-PD-L1/PD-1. Anti-CTLA4 predominantly inhibits T-regulatory cells (Treg cells), thereby increasing the CD8 T-cell to Treg (CD8/Treg) ratio. Radiation enhances the diversity of the T-cell receptor (TCR) repertoire of intratumoral T cells. Together, anti-CTLA4 promotes expansion of T cells, while radiation shapes the TCR repertoire of the expanded peripheral clones. Addition of PD-L1 blockade reverses T-cell exhaustion to mitigate depression in the CD8/Treg ratio and further encourages oligoclonal T-cell expansion. Similarly to results from mice, patients on our clinical trial with melanoma showing high PD-L1 did not respond to radiation plus anti-CTLA4, demonstrated persistent T-cell exhaustion, and rapidly progressed. Thus, PD-L1 on melanoma cells allows tumours to escape anti-CTLA4-based therapy, and the combination of radiation, anti-CTLA4 and anti-PD-L1 promotes response and immunity through distinct mechanisms.
Product Citations
-
PET Imaging of System A Amino Acid Transport Detects Early Response to Immune Checkpoint Inhibitor Therapy in a Syngeneic Mouse Model.
In J Nucl Med on 3 December 2025 by Akca, U., Zhang, Y., et al.
PubMed
Immune checkpoint inhibitor (ICI) therapy is effective and in routine clinical use for various cancers, but accurately identifying which patients will respond remains a significant challenge. The PET agent 18F-FDG has uptake by cancer cells as well as inflammation induced by ICI therapy, complicating and often limiting the utility of 18F-FDG for early response assessment during ICI therapy. An imaging agent that accurately distinguishes responders from nonresponders early in the course of ICI therapy could enable intensification or change of therapy for nonresponders. In this study, the 18F-labeled amino acid 18F-MeFAMP, a fluorinated analog selectively targeting system A amino acid transport, was compared with 18F-FDG in the MC38 syngeneic mouse model of ICI therapy. 18F-MeFAMP was chosen because of the relatively low uptake of system A substrates in inflammatory tissues combined with growing evidence suggesting system A transporters are involved in immunotherapy. Methods: PET/CT imaging was used to compare tumor uptake of 18F-MeFAMP with tumor uptake of 18F-FDG before and 6 d after starting dual ICIs in MC38 tumor-bearing female C57BL/6 mice. SUVs, biologic tumor volumes, and total lesion activity were measured along with selected tumor-to-organ ratios. Histogram analysis of tracer uptake was performed to assess differences in tumor activity distribution between responders and nonresponders. Results:18F-FDG showed no significant differences at baseline or after ICI regardless of response. In contrast, 18F-MeFAMP SUVs defined using a 40% of SUVmax threshold (SUV40%) decreased significantly in responders (-60.0% ± 15.6%, P < 0.0001), whereas nonresponders showed no significant change (+45.5% ± 51.2%, P = 0.09). Similar patterns were observed with SUVmax, biologic tumor volume, and total lesion activity measures with 18F-MeFAMP. Histogram analysis revealed significant 18F-MeFAMP uptake differences between groups before and after imaging (P < 0.05). 18F-MeFAMP demonstrated low uptake in common metastatic sites, including liver, lungs, and brain. Conclusion:18F-MeFAMP better detected early ICI response than 18F-FDG with favorable whole-body imaging properties. These findings support further investigation of 18F-MeFAMP for early evaluation of response to ICI and the role of system A substrates in cancer and immune cells before and during ICI.
-
Prednisolone modulates CD8⁺ and regulatory T-cell activity to dampen response to immune checkpoint inhibitor therapy in melanoma.
In Oncoimmunology on 31 December 2026 by Brown, J. R., Pedersen, B., et al.
PubMed
Immune checkpoint inhibitors (ICIs) have transformed the treatment of advanced melanoma, yet their efficacy is limited by high-grade immune-related adverse events that often require treatment with systemic corticosteroids. Although corticosteroids are widely used, their impact on anti-tumor immunity remains poorly defined. Using an ICI-responsive murine melanoma model, we show that tapered systemic prednisolone administered after three cycles of combined anti-CTLA4 and anti-PD1 therapy compromises ICI-mediated tumor control, leading to delayed progression in one-third of initially responding animals. Mechanistically, prednisolone selectively suppressed CD8+ effector T-cell activation in tumor-draining lymph nodes and in the circulation, while expanding activated regulatory T-cells. These changes increased the Treg:CD8+ effector ratio, reduced cytotoxic T-cell function and blocked the early ICI-mediated induction of cytokines, including IL-2, IFNγ, VEGF, CCL3/4, IL-13, IL-3, and GM-CSF. Importantly, despite these early immunosuppressive effects, long-term tumor-specific memory responses were preserved. Autologous melanoma:T-cell cocultures validated these findings. Overall, systemic prednisolone disrupts early CD8+ T-cell-mediated anti-tumor activity but spares durable immunity, highlighting the critical importance of timing and context in the introduction of corticosteroids during ICI therapy.
-
SAHA Alters Macrophages in the Tumor-Immune Landscape in Preclinical Models of Triple-Negative Breast Cancer.
In Pharmaceutics on 28 April 2026 by Lynch, S. E., Crawford, C. I., et al.
PubMed
Background/Objectives: Histone deacetylase (HDAC) inhibitors have been shown to prime the response to immunotherapy (IMT) treatment by inducing immune activation and infiltration to target tumor cells. Many studies primarily focus on adaptive immune cells and their expression of pro-inflammatory markers, like somatostatin receptor 2 (SSTR2); however, macrophages are known to help mediate key tumor microenvironment changes. The goal of this study is to evaluate the effects of HDAC inhibitors and IMT on macrophages, their expression of SSTR2, and their impact on the treatment response in triple-negative breast cancer (TNBC). Methods: Cytotoxic effects of HDAC inhibitors on 4T1 mouse mammary carcinoma cells, including suberoylanilide hydroxamic acid (SAHA), were evaluated using flow cytometry. Bone marrow-derived macrophages (BMDMs) were stimulated to M1-like and M2-like phenotypes and treated with SAHA to explore the effects on SSTR2 expression in different macrophage phenotypes. 4T1-tumor-bearing BALB/c mice were used to evaluate the therapy response to four treatments: saline control, SAHA, anti-PD-1 + anti-CTLA-4 checkpoint blockade IMT, or a combination of SAHA + IMT. Additional cohorts of 4T1-tumor-bearing BALB/c mice and NOD SCID mice, which lack adaptive immune cells, were euthanized for early evaluation of tumor-associated macrophage (TAM) populations via flow cytometry and cytokine analysis. One-way independent ANOVAs and log-rank tests were used to compare group differences. Results: SAHA promotes SSTR2 expression on M1-like BMDMs in vitro. SAHA promotes M2-like TAMs in vivo and stimulates pro-inflammatory, anti-tumor cytokine production in combination with IMT. Conclusions: SAHA drives SSTR2 expression and anti-tumor innate immune responses with additive effects in combination with immunotherapy in preclinical TNBC.
-
Targeting the novel immune checkpoint KLRG1 is markedly therapeutic against cancer through multiple lymphocyte subsets.
In J Immunother Cancer on 9 April 2026 by Jones, T. A., Shapiro, J. W., et al.
PubMed
Checkpoint blockade therapies have demonstrated clinical benefit across multiple cancer types; however, many patients with immune cell infiltration remain non-responsive or develop resistance. This suggests that additional, unidentified regulatory pathways limit treatment efficacy. The purpose of this study was to investigate the role of the inhibitory receptor KLRG1 in limiting antitumor immunity and to evaluate its potential as a therapeutic target in patients refractory to first-generation checkpoint inhibitors.